Key Takeaways
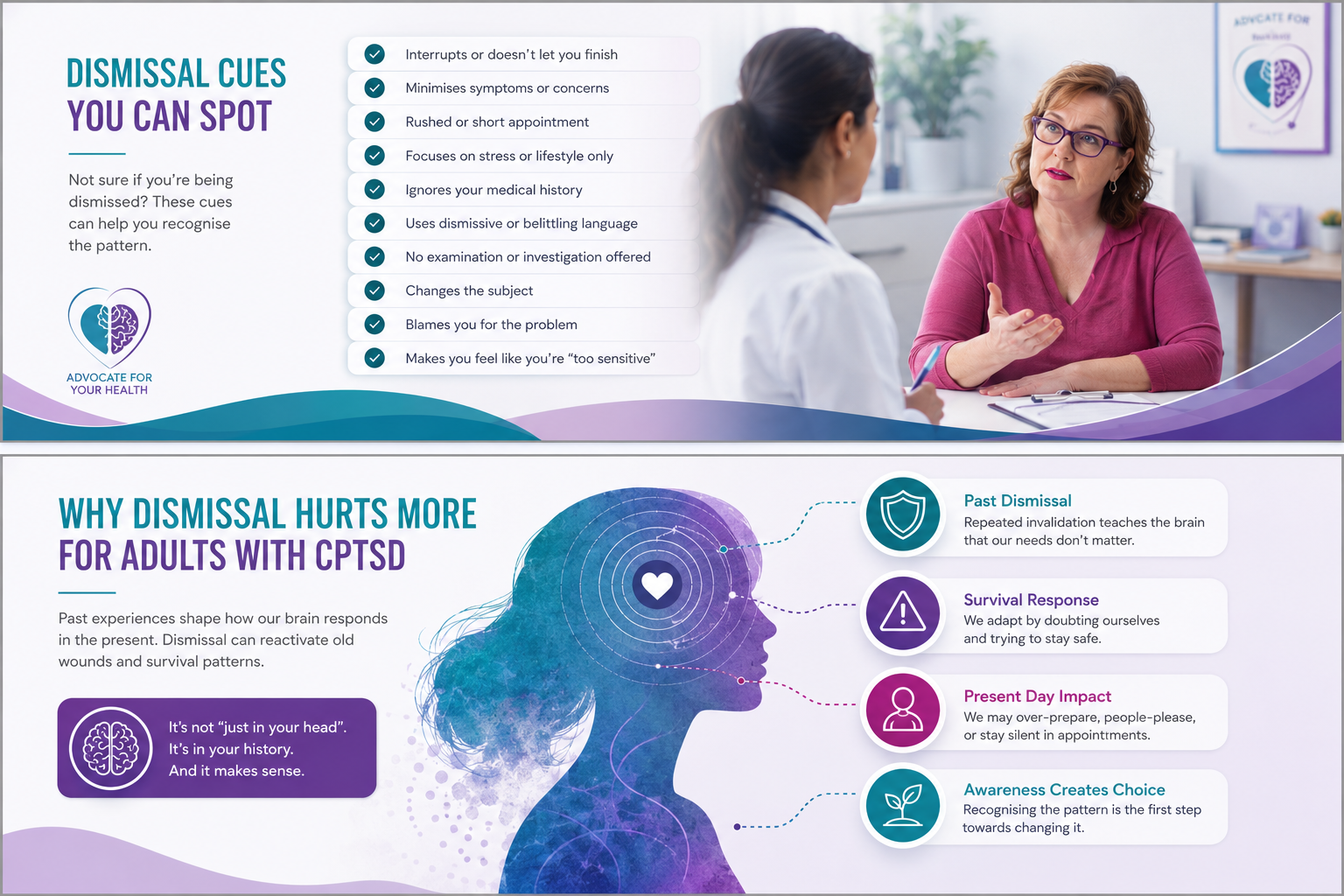
When you leave the appointment and blame yourself first
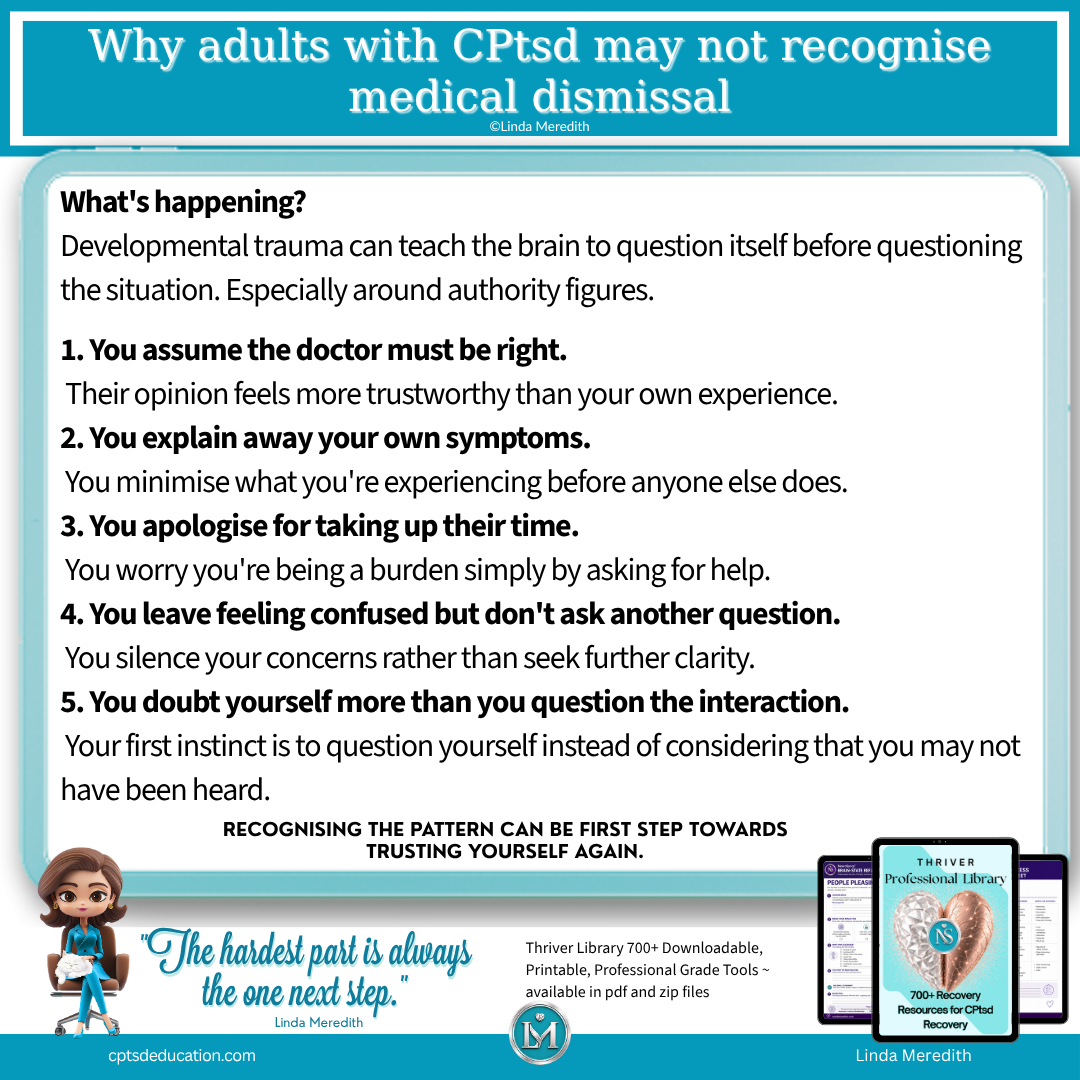
Why CPtsd can make you trust authority over your own body
How medical dismissal can be missed in the moment without blaming clinicians
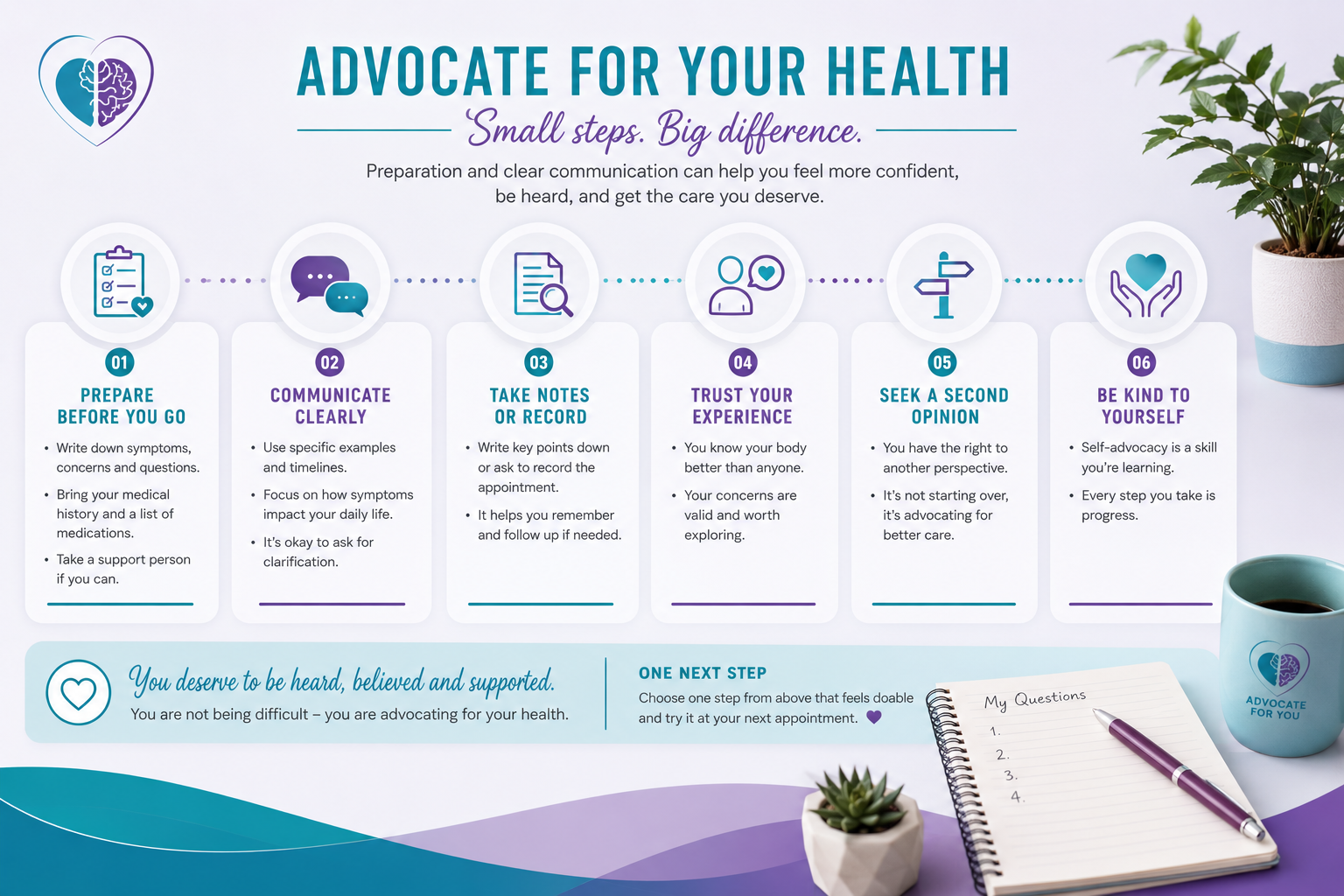
The five common appointment patterns and what to try instead
You assume the doctor must be right
You explain away your own symptoms
You apologise for taking up their time
You leave feeling confused but don’t ask another question
You doubt yourself more than you question the interaction
One Next Step to try before your next appointment
Choose your One Next Step
Education
CPtsd Recovery Libraries
CPtsd Recovery with Linda
References
American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.; DSM-5-TR). American Psychiatric Publishing
Centers for Disease Control and Prevention. (2024). Preventing adverse childhood experiences (ACEs): Leveraging the best available evidence. CDC
Cloitre, M., Garvert, D. W., Weiss, B., Carlson, E. B., & Bryant, R. A. (2014). Distinguishing PTSD, complex PTSD, and borderline personality disorder: A latent class analysis. European Journal of Psychotraumatology, 5, 25097
Dueñas, J. L., et al. (2020). Gender bias in clinical practice guidelines: A systematic review. PLOS ONE, 15(9), e0239324
Elliott, A. M., Alexander, S. C., Mescher, C. A., Mohan, D., & Barnato, A. E. (2016). Differences in physicians’ verbal and nonverbal communication with black and white patients at the end of life. Journal of Pain and Symptom Management, 51(1), 1–8
International Society for Traumatic Stress Studies. (2019). Posttraumatic stress disorder prevention and treatment guidelines: Methodology and recommendations. ISTSS
Kirmayer, L. J., & Rai, S. (2017). Medical anthropology and the study of global mental health. Psychiatric Clinics of North America, 40(2), 315–330
National Institute for Health and Care Excellence. (2018, updated). Post-traumatic stress disorder: NICE guideline (NG116). NICE
Purtle, J. (2020). Systematic review of evaluations of trauma-informed organizational interventions that include staff trainings. Health Services Research, 55(S2), 459–475
Saitz, R., Larson, M. J., LaBelle, C., Richardson, J., & Samet, J. H. (2008). The case for chronic disease management for addiction. Journal of Addiction Medicine, 2(2), 55–65
Samuels, E. A., et al. (2018). “Sometimes you feel like the freak show”: A qualitative assessment of emergency care experiences among patients with chronic pain. Annals of Emergency Medicine, 72(5), 532–541
World Health Organization. (2021). Guidance on community mental health services: Promoting person-centred and rights-based approaches. WHO
Linda Meredith
Passionate, Innovative, and Dedicated to
Complex Trauma Recovery
An Advanced, Neuroscience Based Approach for Mental Health Professionals
NeuroSynqt™ education is peer reviewed and delivered by a Registered Training Provider.
NeuroSynqt™ education is peer reviewed and delivered by a Registered Training Provider.
Supporting integration that addresses intergenerational trauma at its source

