Key Takeaways
When you leave an appointment feeling smaller than when you arrived
Dismissal cues you can spot in the moment
Why it matters more than hurt feelings
Concrete scripts and steps that protect you
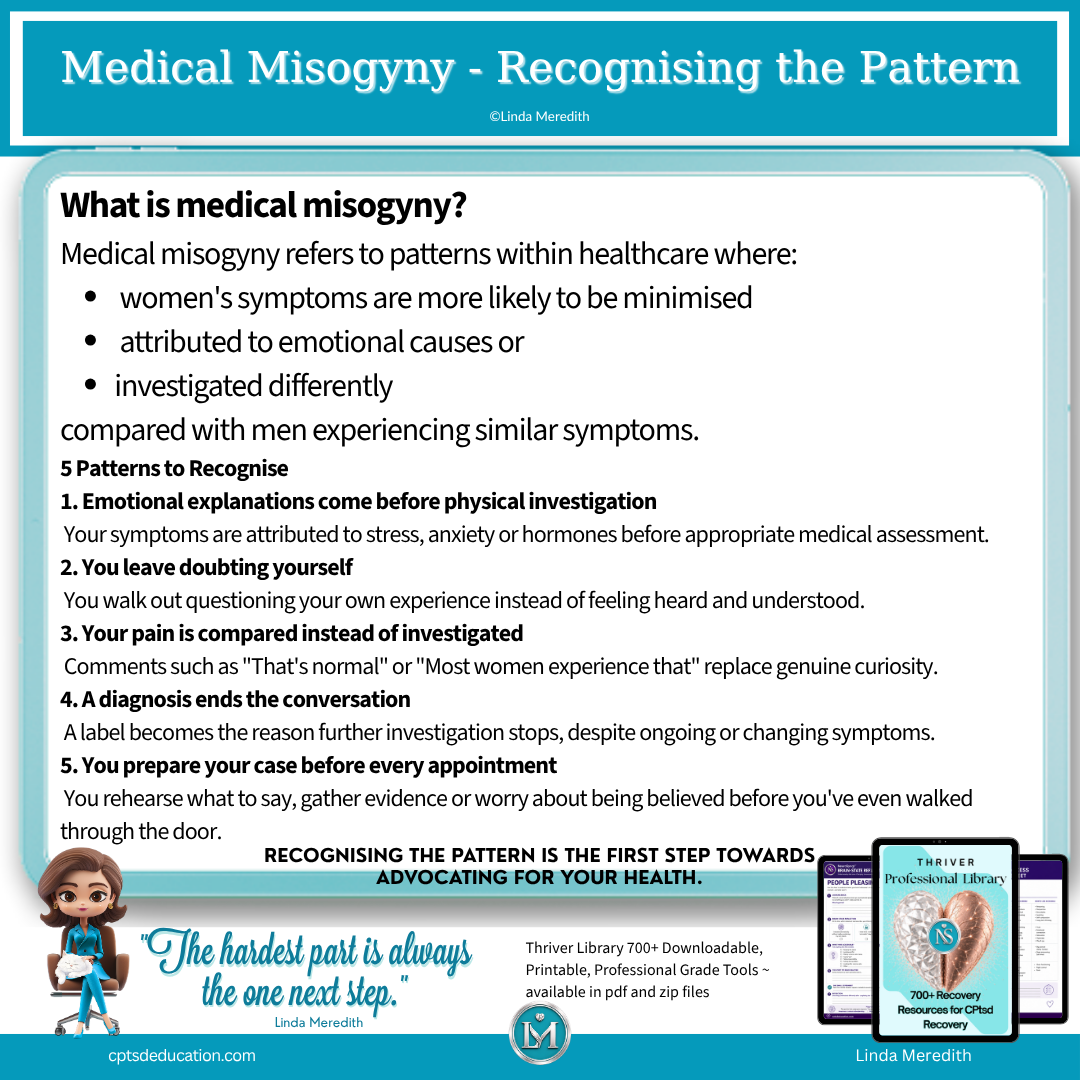
Spotting medical misogyny and dismissal in the room
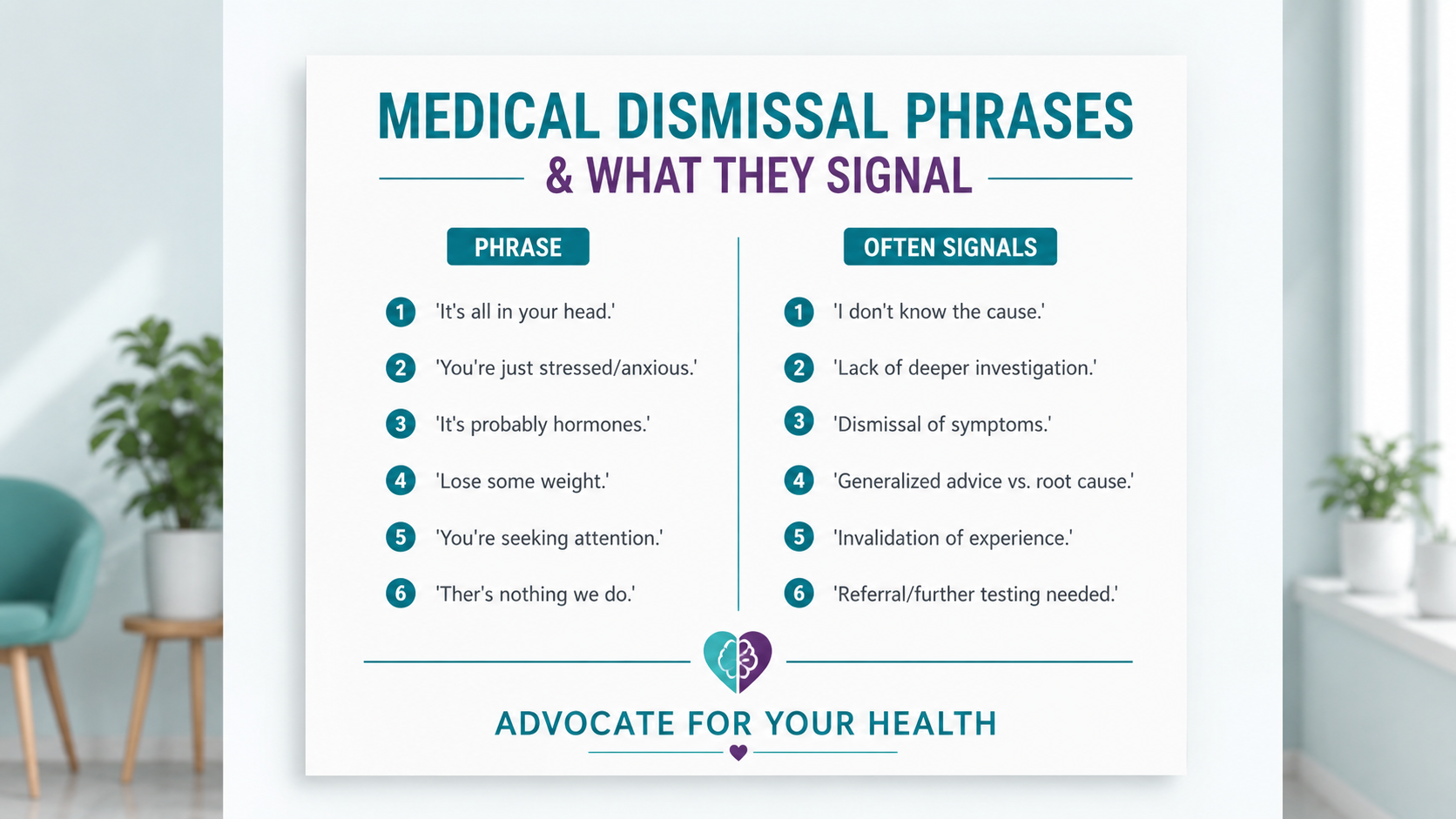
Red flags to listen for in real time
Pattern recognition: when uncertainty turns into blame
Why dismissal hits harder for adults with Complex PTSD

What to do next: safer appointments, better documentation, clearer escalation
Preparation tactics that reduce dismissal
In-appointment scripts you can read verbatim
Escalation that stays factual and keeps you safer
Explore Complex Trauma Trained Certification for working effectively with CPtsd
Choose your One Next Step
Education
CPtsd Recovery Libraries
CPtsd Recovery with Linda
References
Medical misogyny / diagnostic bias
Hamberg K. (2008). Gender Bias in Medicine. Women's Health. 4(3), 237-243.
Samulowitz A, Gremyr I, Eriksson E, Hensing G. (2018). "Brave Men" and "Emotional Women": A Theory-Guided Literature Review on Gender Bias in Health Care and Gendered Norms Towards Patients with Chronic Pain. Pain Research and Management.
Hoffmann DE, Tarzian AJ. (2001). The Girl Who Cried Pain: A Bias Against Women in the Treatment of Pain. Journal of Law, Medicine & Ethics.
Diagnostic delay
World Health Organization. Gender and Health (overview of gender inequities in healthcare).
National Institutes of Health. Research on sex differences in diagnosis and treatment.
Trauma-informed healthcare
Substance Abuse and Mental Health Services Administration. SAMHSA's Concept of Trauma and Guidance for a Trauma-Informed Approach.
Centers for Disease Control and Prevention. Adverse Childhood Experiences (ACEs).
Linda Meredith
Passionate, Innovative, and Dedicated to
Complex Trauma Recovery
An Advanced, Neuroscience Based Approach for Mental Health Professionals
NeuroSynqt™ education is peer reviewed and delivered by a Registered Training Provider.
NeuroSynqt™ education is peer reviewed and delivered by a Registered Training Provider.
Supporting integration that addresses intergenerational trauma at its source

